

Arthritis of the Knee
At Nebraska Hand & Shoulder Institute, P.C., we understand how debilitating knee arthritis can be and are dedicated to providing personalized care to help you regain mobility and improve your quality of life. Whether you’re dealing with arthritis and knee pain or advanced knee joint arthritis, our team offers a range of effective treatment options tailored to your unique needs. From non-surgical approaches like physical therapy and joint injections to advanced knee arthritis surgery, we focus on both pain relief and long-term joint health.
If knee arthritis is impacting your daily life, our expertise in managing joint conditions ensures you receive the most up-to-date care. Whether your goal is to reduce pain or return to your favorite activities, we’re here to guide you every step of the way. Schedule a consultation with our skilled specialists to explore the best treatment options, including knee arthritis surgery, for your specific needs.

Understanding Knee Arthritis
Knee arthritis is a common condition that often develops as we age, leading to knee joint inflammation and difficulty with daily activities. It is typically caused by two main types: degenerative arthritis and inflammatory arthritis. Degenerative arthritis, the most common form, occurs when cartilage in the knee joint wears down over time, causing bones to rub together. Inflammatory arthritis, such as rheumatoid arthritis (RA) and gout, can result from the immune system attacking healthy tissues or the buildup of urate crystals in the joint, leading to significant pain and swelling.
Rising rates of knee arthritis are closely linked to factors like aging and obesity. Excess weight puts extra strain on the knees, accelerating cartilage breakdown and worsening knee joint inflammation. This "obesity tsunami" has caused more individuals to seek ways to treat knee pain and regain mobility. However, even with advancements in knee replacement surgery, many patients do not experience improved activity levels or weight loss afterward.
At Nebraska Hand & Shoulder Institute, P.C., we consider your medical history and lifestyle to offer personalized treatment options. From conservative therapies to advanced surgical care, we work to reduce pain, improve mobility, and help you return to your daily activities with confidence.
Treatment Options for Knee Arthritis
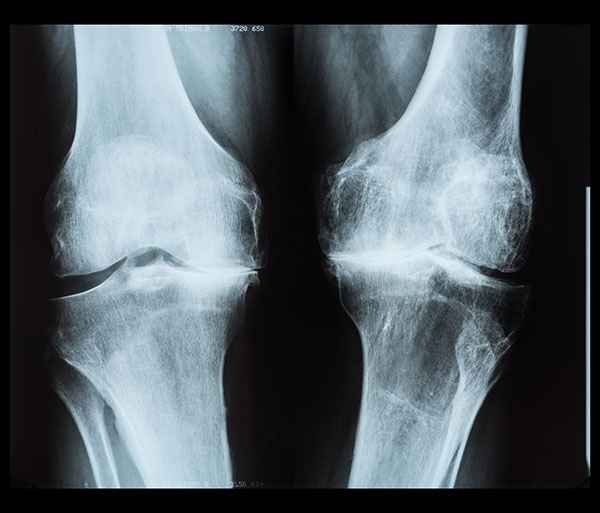
Your doctor will examine your knee and take weight-bearing x-rays to assess cartilage thickness. After examination, a treatment plan will be created based on your personal needs.
Medications for Arthritis
Non-steroidal anti-inflammatory drugs (NSAIDs) are a cornerstone treatment for degenerative arthritis. These medications, derived from the chemical pathway of aspirin, work by reducing inflammation and pain in the joint tissue. Modern NSAIDs, like ibuprofen, are generally safe for most people with normal kidney function, no history of ulcers, and no allergies to NSAIDs. Regular use is necessary, as arthritis cannot be reversed, and new cartilage cannot be generated.
It typically takes four to six weeks to see if NSAIDs are effective for managing your symptoms.
Cortisone Injections
Cortisone injections into the knee can provide rapid and effective pain relief, making them a valuable option for managing acute discomfort or inflammation. The procedure typically involves first withdrawing any excess fluid from the joint to reduce swelling and improve the injection's effectiveness, followed by the administration of cortisone, a powerful anti-inflammatory medication.
While these injections can offer significant short-term relief, they should be used judiciously, with a limit of three to four injections per year. Overuse may lead to potential side effects, such as weakened cartilage, altered calcium metabolism, and an increased risk of joint damage over time. Patients considering this treatment should discuss the risks and benefits to ensure this procedure will be beneficial.
Hyaluronic Acid (HA) Injections
Hyaluronic acid (HA) injections, originally sourced from rooster combs but now synthesized in laboratories, offer an alternative treatment option for certain individuals. These injections may be suitable for those who cannot tolerate NSAIDs; however, they are relatively expensive and have not consistently demonstrated greater effectiveness than cortisone injections or NSAID therapy. Due to their high cost and variable outcomes, HA injections are typically considered a last-resort treatment when other options have been exhausted.
The Role of Mobility Aids
Using a cane can be an effective way to significantly reduce knee pain by providing additional support. When held in the hand opposite the affected knee, a cane can reduce the weight placed on the joint by approximately 50% during walking, alleviating strain and discomfort. However, despite its proven benefits, many individuals are reluctant to use a cane due to societal stigma and a preference for more immediate, less noticeable solutions.
Weight Loss and Surgery
Losing 25 to 50 pounds or more can significantly reduce or even eliminate knee pain by decreasing the stress placed on the joints. Achieving weight loss can be challenging and often requires a multifaceted approach, including lifestyle changes and, in some cases, medical support. For some individuals, incorporating medications designed to aid weight loss, combined with regular exercise and diet changes, can lead to improved outcomes.
In more severe cases, weight-reduction surgery, such as gastric bypass or sleeve gastrectomy, may be an option. These procedures, performed by general surgeons, aim to limit stomach capacity or alter the digestive system to reduce calorie absorption. While these surgeries can lead to substantial weight loss and associated improvements in joint health, they may also introduce challenges. For instance, some patients may develop an intolerance to NSAIDs (nonsteroidal anti-inflammatory drugs) after surgery, which could complicate the management of arthritis and joint pain.
A comprehensive discussion with healthcare providers can help determine the best approach for weight management while addressing any potential implications for joint health and overall well-being.
Final Thoughts
Effective knee arthritis treatment often combines weight management, medication, and mobility aids. While some treatments offer short-term relief, addressing underlying factors like weight and inflammation can lead to more sustainable improvements. Consult your doctor to determine the best approach for your needs.
Joint Replacement
Joint replacement is a good option for those who cannot take anti-inflammatory medications, have not had success with them, and find little relief from occasional cortisone injections or using a cane. Over time, orthopaedists have discovered that the closer an implant matches the natural contour of the joint—whether it's a knee, hip, ankle, or even a finger—the better the results. This ensures maximum motion while reducing the risk of the implant becoming loose. Joint replacement surgery relieves pain by cutting thousands of nerve endings in the joint and covering the joint surfaces with durable materials like high-density polyethylene and cobalt-chrome-molybdenum, similar to how a dentist places a crown on a tooth. These materials rarely cause inflammatory responses and, when properly implanted, can last 25 years or more.
However, joint replacement is usually avoided for individuals under 50 unless they have severe arthritis, as younger patients may place more strain on the implant. While activities like jogging, cycling, or light exercise are generally acceptable, high-impact activities like soccer, football, or forceful pivoting increase the risk of loosening the implant. Following recommended activity guidelines is essential for maintaining the long-term success of joint replacement surgery.
Total Knee Replacement vs Partial Knee Replacement
When considering treatment options for knee arthritis, both total knee replacement (TKR) and partial knee replacement (PKR) are widely performed surgical procedures, each with distinct benefits and drawbacks. Understanding the differences between the two can help patients and medical professionals decide which is most suitable based on individual needs.
Total Knee Replacement (TKR)
First introduced in the 1960s, total knee replacement involves replacing the entire knee joint, including the medial, lateral, and patellofemoral compartments. Early surgeries lacked precision tools, but by the 1980s, improved cutting jigs and advancements in materials like metal alloys, plastics, and bone cement significantly enhanced outcomes. Today, TKR is one of the most common treatments for advanced knee arthritis, with an 83% patient satisfaction rate.
TKR is suitable for cases where arthritis has significantly affected multiple compartments of the knee. However, it does come with some disadvantages. Patients often experience longer recovery times, increased surgical risks such as higher blood loss and the need for transfusions, and sometimes a more restricted range of motion due to ligament removal. Approximately 10% of patients report anterior knee pain after surgery, even when the patella (kneecap) is resurfaced. Some surgeons have opted to avoid resurfacing the patella entirely, which has been shown to reduce costs, pain, and surgery time without compromising outcomes.
Despite its widespread use in the U.S., total knee replacement can result in greater hospital costs, increased waste, and a higher environmental impact compared to its alternative, partial knee replacement.
Partial Knee Replacement (PKR)
Partial knee replacement, first developed in the 1970s, focuses on replacing only the damaged compartment of the knee, typically the medial (inner) or, less commonly, the lateral (outer) compartment. In patients with localized arthritis, PKR offers several advantages over TKR. These include a smaller incision, minimal blood loss, reduced risk of blood clots, and faster recovery times. Unlike TKR, PKR preserves the knee's natural ligaments, allowing for more natural joint movement and better overall mechanics.
Patient satisfaction with PKR tends to be higher, at around 90%, and individuals who have had both a partial and a total knee replacement on opposite knees often prefer the side with the partial procedure. This is particularly true in the UK, where partial knee replacements are more widely accepted and performed with excellent long-term results.
One of the reasons PKR has not gained the same level of popularity in the U.S. is due to historical misconceptions. A 1989 study published in the Journal of Bone and Joint Surgery (JBJS) from Brigham and Women’s Hospital provided misleading information about PKR’s effectiveness, influencing surgeons and patients alike. Additionally, due to the slightly higher complexity of the procedure and lower reimbursement rates compared to TKR, many surgeons in the U.S. have been slow to adopt PKR.
Key Considerations for PKR
Research has disproven earlier beliefs that arthritis in one part of the knee, such as the medial compartment, would inevitably spread to other compartments. Studies from the U.S. have shown that over 50% of knee arthritis patients are viable candidates for PKR, far exceeding the outdated estimate of 5%. Even in cases where there is mild arthritis in other compartments, PKR can still be a viable option by removing bone spurs and addressing minor nerve issues during surgery.
British surgeons have classified medial compartment arthritis as a distinct condition—anteromedial degenerative arthritis—that rarely progresses to other areas of the knee. This is supported by the longevity of PKR results in the UK. For patients with localized arthritis, PKR provides a less invasive solution with long-term benefits.
Environmental and Cost Implications
In addition to the medical benefits, PKR also has advantages in terms of cost and environmental impact. Because it requires fewer resources, involves less hospital waste, and has a shorter recovery period, PKR is a more sustainable and cost-effective treatment. As concerns over global warming and waste management grow, PKR offers an environmentally conscious alternative for eligible patients.
Which Option is Right for You?
The choice between total and partial knee replacement ultimately depends on the extent of arthritis and the patient’s overall health. TKR may be necessary for patients with widespread arthritis affecting multiple compartments, while PKR is ideal for those with localized damage. Patients considering their options should discuss the benefits, risks, and long-term outlook of each procedure with their surgeon to determine the best approach for their individual condition.
By understanding the distinctions between TKR and PKR, patients and surgeons can make better-informed decisions, improving outcomes and quality of life for those living with knee arthritis.

Who is a candidate for knee replacement, uni or total?
Candidates for knee replacement surgery are typically individuals with severe degenerative arthritis unresponsive to treatment, who are otherwise healthy enough for spinal or general anesthesia. Diabetics must have well-controlled blood sugar levels (A1c near normal) to minimize infection risk, as infections following joint replacement significantly lower life expectancy and increase costs.
Cruciate ligaments (ACL and PCL) are vital for knee stability. Partial knee replacements (uni knees) require intact cruciates, while total knee replacements can compensate for their absence, with some surgeons opting to remove both cruciates for easier implant placement. Patients with inflammatory arthritis (e.g., rheumatoid arthritis) are not suitable for partial knee replacements due to the disease affecting the entire joint, often leading to further damage in untreated areas.
Severe knee deformities and advanced joint damage require total knee replacements, as partial replacements cannot correct significant deformities. Obesity and uncontrolled diabetes increase the risks of blood clots, infection, and complications during surgery. While obesity complicates the procedure, its impact on implant loosening remains unclear.
Risks
The risks of undergoing a knee joint replacement are bleeding, infection, and blood clots of the calf or upper thigh area that could migrate up to the lungs, i.e., pulmonary embolus, which can be fatal in a number of people. These risks have to be weighed against the benefit of pain relief, increased mobility, cutting down some medication that was being taken for pain and/or inflammation, and allowing those people who really want to become more active, admittedly a minority.
Generally, a joint replacement for arthritis does not improve motion substantially. In fact, most patients who undergo a total knee replacement lose motion and end up with an average of about 105 degrees of flexion, the minimum amount to properly go up and down stairs. Normal knee motion is from 0 to 135-140 degrees. Thus, there is about a 35-degree loss of knee motion in many patients related to scarring and inactivity. At the time of surgery, the surgeons clearly demonstrate tremendous motion. Habitually inactive patients allow the “new knee” to become stiff regardless of the amount of physical therapy attended. Unicompartmental knee replacement does not affect knee motion. It possibly increases it in people just by eliminating pain, but because the ligaments are allowed to remain, one is just removing arthritis on one side of the knee. Much like putting a crown on a tooth. The mechanics of the knee are not changed.
Summary and Conclusion
At Nebraska Hand & Shoulder Institute, P.C., our knee arthritis doctor provides advanced treatment options tailored to each patient’s unique needs. For those experiencing arthritis of the knee, we offer evidence-based alternatives to total knee replacement, including partial-knee replacement. This type of surgery often delivers effective pain relief, fewer side effects, and equal longevity, all with a lower risk compared to traditional procedures.
We focus on helping patients strengthen the muscles around the knee to support mobility and reduce pain, while also addressing various forms of arthritis. Our team works closely with patients to explore all available options, ensuring the best possible outcomes and avoiding unnecessary surgeries. At Nebraska Hand & Shoulder Institute, P.C., we're dedicated to improving lives with the highest quality care for knee arthritis.