

Expert Ganglion Cyst Treatment in Nebraska
Relief for Hand and Wrist Lumps at Nebraska Hand & Shoulder Institute, P.C.
A ganglion cyst is one of the most common causes of a lump on the wrist or hand. These soft, fluid-filled, non-cancerous swellings account for over 50% of all hand and wrist masses. Ganglion cysts may be painless or cause discomfort, especially when they grow large or press on nearby nerves or tendons.
At Nebraska Hand & Shoulder Institute, P.C., our specialists offer personalized evaluation and treatment options for both hand ganglion cysts and wrist ganglion cysts, from conservative care to advanced surgical solutions.
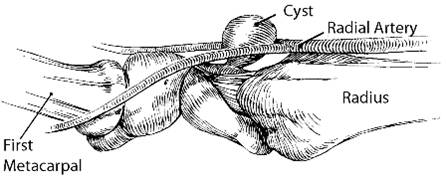
Diagram of a wrist ganglion cyst (as seen from the side with the wrist turned palm upwards)
Understanding the Ganglion Cyst
A ganglion cyst is a round or oval lump that typically develops near a joint or tendon, most often in the wrist, hand, or fingers. Inside the cyst is a thick, jelly-like fluid. These cysts may appear suddenly or develop slowly over time.
Ganglion cysts are:
- Usually benign (non-cancerous)
- Most common on the top of the wrist, the thumb side of the hand, or the end joints of the fingers
- Often solitary but can occur in multiple locations
They tend to affect individuals between the ages of 10 and 40, and are more common in women. There’s no known link to job type or lifestyle.

Ganglion Cyst Causes and Symptoms
A ganglion cyst forms when fluid from a nearby joint or tendon sheath leaks into surrounding tissue. This may occur due to degeneration of the joint capsule or connective tissue, sometimes in association with arthritis. The cyst is often connected to the joint by a narrow stalk that functions like a one-way valve, allowing fluid to enter but not return.
Some ganglia, particularly mucous cysts, develop in response to degenerative arthritis at the end joints of the fingers. These can cause fingernail deformities, and if left untreated, they may rupture and become infected.
Advanced degenerative arthritis at the end joint of the finger (DIP joint) frequently results in a cyst known as a mucous cyst and may cause significant nail deformity.

Cyst caused by arthritis

Cyst at nail fold that has popped

Pressure from a cyst just above the nail fold has caused a deep trough in the nail. Removal of the cyst will allow the nail to grow back normally in about 4 months.
WARNING: MAY CONTAIN GRAPHIC IMAGES
Symptoms
The symptoms of a ganglion cyst can vary:
- A visible lump on the wrist or hand
- Pain or aching, especially with motion or pressure
- Weakness or limited range of motion in the hand or wrist
- In some cases, the cyst is completely painless
Ganglion cysts may grow gradually or seem to appear overnight. Some resolve on their own—up to 58% disappear spontaneously in some studies.
When to Seek Treatment
You may not need treatment if the cyst is small and doesn’t cause symptoms. However, you should consult a specialist if:
- The cyst causes pain, weakness, or discomfort
- It affects your ability to use your hand or wrist
- You’re unsure whether the lump is a ganglion cyst or something else
- You’re concerned about the appearance of the lump
Ganglion Cyst Diagnosis and Treatment Options
In most cases, a ganglion cyst can be diagnosed through a simple physical examination. The cyst’s classic location, size, and feel—typically a round, soft, or firm lump—are usually enough to confirm the diagnosis. Most often, the cyst is found on the back or side of the wrist, hand, or finger joints.
If necessary, X-rays may be taken to:
- Identify any underlying arthritis
- Rule out bone tumors or other conditions
- Look for joint-related causes behind the lump
Non-Operative Treatment
Non-Operative Treatment
Not all ganglion cysts require treatment—especially if they are small, painless, and not interfering with function.
Here are common non-operative options:
- Observation - Many cysts are harmless and may shrink or go away on their own. If the cyst isn’t causing discomfort, it may be safe to simply monitor it over time.
- Aspiration (Draining the Fluid) - Involves drawing the jelly-like fluid from the cyst with a needle. While this may temporarily reduce the size, recurrence is common because the cyst lining and connection to the joint remain.
- Cortisone Injections - Occasionally used to reduce inflammation, though they don’t address the root cause. In clinical experience, recurrence rates are high, and the treatment is often ineffective in the long term.
- Home Remedies or Popping the Cyst - Trying to rupture the cyst by applying pressure or striking it—sometimes called “Bible therapy”—is outdated and not recommended. This method is unreliable and may lead to complications.
In most cases, nonsurgical treatment is best for cysts that are not painful, not growing, and don’t interfere with hand or wrist movement.
Surgical Treatment for Ganglion Cysts
If a ganglion cyst is large, painful, interfering with hand function, or positioned in a location that causes frequent irritation (such as on the wrist or near nerves), surgery to remove the cyst may be the most effective and long-lasting solution.
Surgical removal, also called an excisional biopsy, involves removing the entire cyst, including its stalk and the portion of the joint capsule or tendon sheath it’s connected to. This reduces the risk of recurrence and provides a permanent resolution in most cases.

Example of a mucous cyst

Nail deformity from a mucous cyst
Wrist Ganglion Cyst Surgery (Traditional Approach)
For a wrist ganglion, surgery is typically performed using a small 1/2-inch transverse incision. The surgeon carefully exposes the cyst down to its origin in the joint, then removes it along with a small wedge of joint capsule. This helps minimize the chance of the cyst returning.
Surgery is performed in an operating room to protect surrounding soft tissue, including superficial nerves and arteries. This approach also allows for precise dissection and reduces the risk of complications.
Arthroscopic Wrist Surgery
In some cases, arthroscopic ganglion cyst wrist treatment may be an option. This technique uses two small puncture incisions and a fiber-optic camera to remove the cyst from inside the joint.
Benefits of arthroscopic surgery include:
- Smaller scars
- Faster recovery
- Similar success rates to open surgery
However, the procedure is more expensive due to specialized equipment and may not be necessary in every case.
How Effective Is Ganglion Cyst Surgery?
Surgical removal is highly effective, with success rates ranging from 85% to 90%. Performing the procedure in a controlled surgical environment ensures safer removal and lowers the risk of damage to nearby structures.
- Most patients recover quickly with minimal post-op discomfort
- There is rarely a need for formal hand therapy
- Early movement is encouraged to prevent stiffness
Post-Surgical Care and Rehabilitation
Recovery from ganglion cyst surgery is typically smooth, with most patients experiencing minimal discomfort and a quick return to normal activities.
At Nebraska Hand & Shoulder Institute, P.C., we use techniques that minimize trauma to surrounding soft tissue, allowing for a faster, more comfortable healing process. After you’ve undergone ganglion cyst removal, we focus on preserving strength and mobility throughout recovery.
Get Expert Ganglion Cyst Care You Can Trust
If you’re dealing with a hard lump on your wrist, hand, or finger, don’t wait and wonder—get clarity and care from a trusted specialist. At Nebraska Hand & Shoulder Institute, P.C., our experienced team provides personalized evaluation and ganglion cyst hand treatment tailored to your needs.
Whether you're looking to confirm a diagnosis, explore non-surgical options, or move forward with surgery to remove a ganglion cyst, we’re here to help. Our patients benefit from decades of surgical expertise and a proven track record of successful outcomes.
Schedule your appointment with a ganglion cyst doctor today and take the first step toward relief and confidence.
Barnes WE, Larson RD, Posch JL: Review of ganglia of the hand and wrist with analysis of surgical treatment. Plastic and Reconstructive Surgery 1964;34:570-574.
Boyes JH. Surgery of the Hand. Philadelphia: Lippicott JB. 1970;5:669
Eaton RG, Dobranski AI, Littler JW: Marginal osteophyte excision in treatment of mucous cysts. J Bone Joint Surg Am 1973;55:570-574.
Flynn JE. Hand Surgery. Baltimore. Williams and Wilkins. 1982:898-902.
Gingrass MK, Brown RE, Zook EG: Treatment of fingernail deformities secondary to ganglions of the distal interphalangeal joint. J Hand Surg [Am] 1995;20:502-505.
Gunther SF: Dorsal wrist pain and the occult scapholunate ganglion. J Hand Surg [Am] 1985;10:697-703.
Kleinert HE, Kutz JE, Fishman JH, McCraw LH: Etiology and treatment of the so-called mucous cyst of the finger. J Bone Joint Surg 1972;54A:1455-8.
McEvedy BV: The simple ganglion: a review of modes of treatment and an explanation of the frequent failures of surgery. Lancet I 1956:135-136.
Nelson CL, Sawmiller S, Phalen GS. Ganglia of the wrist and hand. J Bone Joint Surg 1972;54A:1459-1464.
Richman JA, Gelberman RH, Engber WD, Salamon PB, Bean DJ: Ganglions of the wrist and digits: Results of treatment by aspiration and cyst wall puncture. J Hand Surg [Am] 1987;12:1041-1043.
Rizzo M, Beckenbaugh R: Treatment of mucous cysts of the fingers: Review of 134 cases with minimum 2-year follow-up evaluation. J Hand Surg 2003;28,3:519-524.
Soren A. Archives of Orthopaedic Trauma Surgery 1982;99,4:247-252
Soren A: Pathogenesis and treatment of ganglion. Clinical Orthopaedics 1963;48:173 179.
Watson, HK: Re-evaluation of the cause of the wrist ganglion. J Hand Surg 1989;14A,5:812- 817.
Young L, Bartell T, Logan SE: Ganglia of the hand and wrist. Southern Medical J 1988;81.6:751-760.
Zubowicz VN, Ishii CH: Management of ganglion cysts of the hand by simple aspiration. J Hand Surg [Am] 1987;12:618-620.