

Two Classifications of Shoulder Pain
The overwhelming majority of people treated for shoulder pain are treated because of irritation or non-traumatic damage to the rotator cuff. Bone prominence due to arthritis is often the cause of pain. Arthritis may also be the primary problem.
Traumatic - Those problems that occur because of injury

Non-Traumatic - Spontaneously occurring processes that we have no control over
WARNING: MAY CONTAIN GRAPHIC IMAGES
Shoulder Function
Ultimately, the function of the shoulder is to position the hand. Complaints regarding the shoulder go something such as “I can’t get my hand behind my back/unclasp my bra”; “I can’t get my hand behind my head”; or “I can’t reach above my head”. The patient will also frequently complain of inability to sleep due to pain.
Anatomy of the Shoulder
“Shoulder” is a general term covering a broad group of muscles in the upper extremity. The bulk of the problems relate to the humerus (upper arm), the scapula (shoulder blade), the prominent projection off of it (acromion) and the four rotator cuff muscles. The deltoid muscle rarely has a problem. From a surgical perspective it just gets in the way of helping to solve the problem because it has to be pulled out of the way to work on the deeper rotator cuff or the shoulder joint (glenohumeral joint).
The trapezius, lattissimus dorsi, levator scapulae, rhomboid, serratus anterior muscle and the teres major and teres minor muscles are important muscles acting upon the scapula and the humerus respectively. These stabilize and strengthen the directions of motions of the other muscles. These muscles sometimes serve as spare parts because there is a fair amount of redundancy. The motions described in the shoulder that doctors record when evaluating a person for a shoulder problem are flexion, extension, internal and external rotation, abduction and adduction and combinations of these motions that make the shoulder such an incredibly versatile joint.
The main arterial blood supply comes off of the subclavian artery.
Innervation of the shoulder muscle includes:
Cranial nerve XI (spinal accessory nerve) which innervates the trapezius muscle
Thoracodorsal nerve (C6-C8) which innervates the latissimus dorsi
Long thoracic nerve which innervates the serratus anterior muscle
Axillary nerve is the exclusive innervation of the deltoid muscle
Suprascapular nerve is the predominant source of innervation of the rotator cuff muscle as well as about 75% of the sensation coming out of the shoulder.
This patient has severe infraspinatus and teres minor muscle atrophy in the left shoulder related to entrapment of the suprascapular nerve (C5 innervated).
Skeleton of the Shoulder
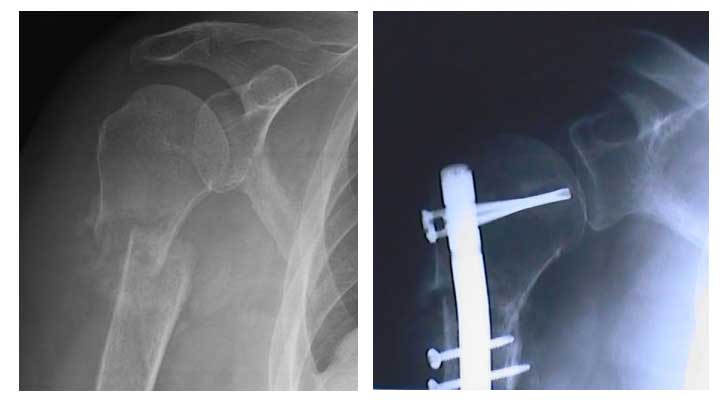
The collar bone (clavicle) originates off the breast bone (sternum). It attaches to the inner side of the long projection coming up the upper side of the scapula known as the acromion. This creates the acromioclavicular (AC) joint. It is a frequent site of pain in a person who falls and lands on the shoulder particularly in football, etc. If there is enough force a person will either sprain the acromioclavicular joint or fracture (break) the clavicle. In people over the age of 40 in particular it is a common site of degenerative arthritis that is often painful.
Rotator Cuff and Shoulder Muscles
The rotator cuff is comprised of the subscapularis, supraspinatus, infraspinatus and the teres minor muscles. These muscles all originate to some degree off of the scapula, or shoulder blade.
Muscles become tendinous at just about the level of the main joint known as the glenohumeral joint. These muscles perform the important function of stabilizing the humeral head which is fairly round but asymmetric in the glenoid which is a slightly concave dish. It is surprising how small the glenoid is compared to the humeral head, thus it is a balancing act.
The labrum is what could best be construed as a retaining wall surrounding the rim of the glenoid and thus, extending its reach. The glenoid labrum is very similar in appearance to the meniscus of the knee. It has become a controversial issue when dealing with rotator cuff pathology and shoulder instability issues common with throwing sports and overzealous athletes.