

Knee Injury Treatment Near You
If you are searching for knee injury treatment near you, Nebraska Hand & Shoulder Institute, P.C. provides expert care guided by an experienced knee pain doctor. Each knee injury is carefully evaluated to determine the most appropriate treatment plan based on your condition, activity level, and long-term mobility goals.
Patients seeking knee pain treatment benefit from advanced diagnostic evaluation, access to specialized knee injury doctors, and treatment options that include non-surgical care as well as minimally invasive procedures using modern arthroscopic techniques. Early evaluation by a knee specialist can help reduce pain, protect joint function, and support a more efficient recovery.
Understanding Knee Injuries
Although the knee is often described as a relatively simple joint, it plays a critical role in weight-bearing, movement, and stability. Knee injuries can affect cartilage, ligaments, or surrounding structures and may result from sports activity, overuse, trauma, or age-related wear.
Because of the knee’s function and constant use, accurate diagnosis and treatment by a qualified knee pain doctor are essential. Advances in diagnostic imaging and arthroscopic techniques allow knee pain specialists to evaluate injuries more precisely and recommend treatment options that align with each patient’s condition and activity level.
Our Knee Treatment Services
At Nebraska Hand & Shoulder Institute, P.C., we provide comprehensive knee injury treatment designed to address both acute injuries and chronic knee conditions. Our knee specialists evaluate each patient individually to determine the most appropriate course of care based on symptoms, activity level, and long-term joint health.
Our knee treatment services include:
- Treating knee injuries related to sports, trauma, and overuse
- Treating anterior knee pain
- Managing knee arthritis
- Providing knee replacement surgery when appropriate
Don’t let knee pain limit your mobility or quality of life. Consult with a knee injury doctor near you to explore personalized treatment options and long-term relief.
Meniscal Injury
A meniscal injury involves damage to the meniscus, which is a wedge-shaped piece of cartilage that helps cushion the knee and distribute weight across the joint. Each knee contains two menisci: the medial (inner) meniscus and the lateral (outer) meniscus. These structures play a critical role in knee stability and function.
Meniscus tears commonly occur due to shearing stress when the knee is bent and twisted. They are especially common in active individuals over the age of 35, as age-related changes in the cartilage can make the meniscus more vulnerable to injury.
Types of Meniscus Tears
Meniscus tears can occur in several patterns, depending on the direction and extent of the damage. The most common types of meniscus tears include:
- Complex tears
- Bucket-handle tears
- Radial/ tears
Each type of tear can affect knee stability and movement differently, which is why accurate diagnosis is important when determining the most appropriate treatment approach.
Meniscus tears commonly cause joint line pain, localized tenderness, and difficulty walking, which may result in a limp. These symptoms can vary depending on the size and location of the tear.
X-rays are often used to rule out fractures or other bony injuries, while nonsteroidal anti-inflammatory medications (NSAIDs), such as meloxicam, may help reduce pain and inflammation. In some cases, particularly with degenerative meniscus tears or persistent symptoms, further evaluation and treatment using arthroscopic techniques may be recommended.
Treatment Options for Meniscal Injury
Treatment for a meniscal injury depends on the type of tear, severity of symptoms, and overall knee stability. In many cases, non-surgical treatment is recommended initially unless symptoms persist or knee function is significantly affected.
Partial Meniscectomy
Partial meniscectomy is commonly recommended for degenerative meniscus tears. This minimally invasive outpatient procedure involves trimming the damaged portion of the meniscus. Post-procedure discomfort is usually limited and may last up to three months.
Meniscal Repair
Meniscal repair is performed when the tear is suitable for repair, which occurs in approximately 10% of cases and is often associated with ACL injuries. This procedure uses sutures to repair the torn meniscus and may require the use of a knee immobilizer and restricted weight-bearing during the recovery period.
Non-Surgical Treatment
Non-surgical options, including rest and nonsteroidal anti-inflammatory medications (NSAIDs), are typically recommended before considering surgery, unless symptoms continue or worsen.
Recuperation from Meniscal Surgery
Arthroscopic meniscectomy has been widely used since the 1980s and is a common treatment for meniscal injuries. This procedure typically results in minimal discomfort along the joint line, with symptoms often resolving within three months.
Meniscal repairs that involve sutures may lead to greater post-operative discomfort and usually require the use of a knee immobilizer along with restricted weight-bearing for several weeks. Following either procedure, patients are advised to avoid running, jumping, and sports activities for at least six weeks. Full recovery generally occurs within three to six months, depending on the procedure performed and individual healing response.
Knee Ligament Injury
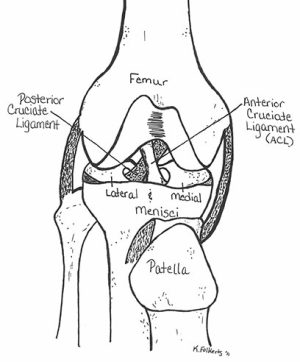
Knee ligament injuries are common, particularly during sports and physical activity, and can range from mild sprains to complete ligament tears. The knee is supported by four primary ligaments: the medial collateral ligament (MCL), lateral collateral ligament (LCL), anterior cruciate ligament (ACL), and posterior cruciate ligament (PCL). The menisci also play an important role in knee stability by acting as weight-bearing cartilage within the joint.
Age can influence how knee injuries present. In adolescents, similar forces may result in growth plate injuries, while adults exposed to the same stress are more likely to sustain ligament tears.
Ligament Injury Grades
Knee ligament injuries are classified into three grades based on the severity of the damage. Identifying the grade of injury helps guide appropriate treatment and recovery expectations.
Grade 1: Mild ligament injury
Grade 1 injuries involve minor damage to the ligament fibers without loss of knee stability. Swelling is minimal, and healing typically occurs within 3 to 6 weeks, often with the use of bracing.
Grade 2: Moderate ligament injury
Grade 2 injuries involve partial tearing of the ligament fibers. These injuries often cause noticeable swelling, pain during stress testing, and mild instability of the knee.
Grade 3: Severe ligament injury
Grade 3 injuries involve a complete ligament tear and result in significant knee instability. Pain may lessen after the initial injury. These injuries are often associated with ACL and meniscus damage, sometimes referred to as the “terrible triad.”
Treatment recommendations depend on the patient’s age, activity level, and the specific ligament involved.
Treatment of Knee Ligament Sprains
Treatment for knee ligament sprains varies depending on the severity of the injury and whether other structures, such as the meniscus or ACL, are involved. Management may range from conservative home care to surgical intervention.
Grade 1: Mild ligament sprain
Treatment typically includes an Ace wrap, ice, and anti-inflammatory medications such as ibuprofen or meloxicam. Walking is generally permitted, but running and jumping should be avoided for approximately three weeks. Gentle cycling and straight-leg raises (quad sets) can help maintain muscle strength during recovery.
Grade 2: Moderate ligament injury
A hinged knee brace or knee immobilizer is often recommended to support the joint and help prevent muscle wasting. Straight-leg raises (quad sets) should be performed several times daily without added weights. Recovery at this stage focuses on maintaining stability and preserving muscle strength.
Grade 3: Severe ligament tear
For grade 3 injuries, it is important to determine whether the injury is isolated or involves additional damage to the meniscus or ACL.
Isolated medial collateral ligament (MCL) tears are commonly treated without surgery using a hinged knee brace for six to twelve weeks. Full weight-bearing is typically allowed as tolerated, although a cane may be necessary during the early stages of recovery.
Anti-inflammatory medications and quad sets remain important components of treatment. If a meniscus tear is present, arthroscopic surgery may be required to repair it. When both the ACL and meniscus are injured, combining ACL reconstruction with meniscus repair helps reduce the risk of re-tearing. ACL tears generally require reconstruction using a tendon graft.
Early diagnosis and an individualized treatment plan are essential for achieving the best possible outcome.
Anterior Cruciate Ligament Injury (ACL)
Anterior cruciate ligament (ACL) injuries are common and often cause significant swelling, pain, and knee instability. These injuries typically involve a complete (grade 3) ligament tear and are associated with meniscus damage in approximately 50% of cases.
Early diagnosis plays an important role in treatment planning. Physical examination techniques such as the Lachman test and pivot shift test are most accurate shortly after the injury occurs. When diagnosis is delayed or when additional injury is suspected, an MRI may be used to evaluate the ACL and menisci.
At Nebraska Hand & Shoulder Institute, P.C., we specialize in the evaluation and treatment of ACL injuries. While ACL reconstruction is not required for every patient, it is often recommended for active individuals, including teenagers and athletes, to restore knee stability and reduce the risk of long-term joint damage. Treatment plans are tailored based on activity level, lifestyle, and injury severity and may include non-surgical management with rest, ice, and physical therapy or surgical reconstruction when full knee function needs to be restored.
Whether you are a competitive athlete or focused on maintaining mobility in everyday activities, our team is committed to guiding you through recovery with personalized ACL injury treatment.
Posterior Cruciate Ligament Injury (PCL)
The posterior cruciate ligament (PCL) is injured far less frequently than the anterior cruciate ligament. Diagnosis can be challenging, as physical examination findings are often similar to those seen with ACL injuries. In many cases, an MRI scan is required to accurately assess the PCL.
Symptoms of a PCL injury may be vague, and outcomes following reconstructive treatment are generally less predictable than those for ACL reconstruction. In most situations, the ACL and PCL are not injured at the same time, except in cases of knee dislocation, where all four major knee ligaments may be torn. Knee dislocations are rare but represent serious injuries.
A significant number of knee dislocation cases are associated with injury to the popliteal artery, which can place the limb at risk if not diagnosed and treated promptly.
Collateral Ligament Injury
Most patients do not experience long-term symptoms following a medial collateral ligament (MCL) injury, even in cases classified as grade 3. Some individuals may notice occasional soreness or mild increased laxity, but these symptoms typically do not lead to lasting knee problems.
Recovery time varies based on the severity of the injury. Grade 1 collateral ligament injuries usually heal within approximately six weeks. Grade 3 injuries may require three to six months for full recovery, with grade 2 injuries falling somewhere between these timelines. Diagnosis is generally made through a physical examination, with X-rays used to rule out an associated fracture.
Anterior and Posterior Cruciate Ligament Injuries
Severe knee swelling that develops within an hour of injury often indicates damage to the cruciate ligaments. Initial treatment typically includes ice and an Ace wrap to help manage swelling, although pain can be significant. In some cases, draining blood from the knee after the first day may help relieve discomfort. During the following week, restoring knee motion becomes a primary focus. If instability persists, particularly during athletic activity, surgical treatment may be necessary, especially when a meniscus tear is also present.
When ACL reconstruction is required, the procedure is most commonly performed using the patient’s own tissue, such as the patellar tendon, quadriceps tendon, or hamstring tendons. Cadaver grafts, also known as allografts, are another option. While allografts carry a very low risk of rejection or disease transmission, may reduce post-operative pain, and can shorten surgery time, using the patient’s own tissue generally produces better long-term outcomes.
Following reconstruction, the repaired tendon initially has good strength but gradually weakens for approximately one year as it heals. Full strength typically returns around 12 months after surgery. During the first six months of recovery, patients should avoid jumping or pivoting activities, although light running on flat surfaces may begin after about six weeks. Accelerating recovery too quickly, as sometimes seen in professional athletes, increases the risk of re-injury and is not medically recommended.
When to See a Knee Specialist Near You
If you are experiencing ongoing knee pain, swelling, instability, or difficulty returning to normal activities, it may be time to consult a knee specialist near you. Early evaluation by an experienced knee injury doctor can help identify the underlying cause of your symptoms and guide appropriate treatment before further joint damage occurs.
You should consider seeking knee injury treatment near you if knee pain persists despite rest, limits daily movement, or interferes with work, sports, or physical activity. Prompt diagnosis and individualized care can improve recovery outcomes and help prevent long-term complications.
Take the Next Step in Your Recovery
Your knee health plays an important role in staying active and maintaining your quality of life. At Nebraska Hand & Shoulder Institute, P.C., we provide expert care for everything from knee pain treatment to advanced knee surgery, guided by experienced knee specialists.
Whether you are looking for a knee pain specialist near you, an orthopaedic doctor for knee pain, or effective knee injury treatment near you, our team is here to help you move forward with confidence. If you have experienced a knee injury, trust our knee injury doctors to provide personalized care focused on recovery and long-term joint health.
Schedule your appointment today to take the first step toward lasting relief.